
Addictions, fatigue, musculoskeletal disorders: how to build a modern occupational health policy
- Marc Duvollet
- Mar 5
- 3 min read


In many companies, occupational health is still reduced to preventing visible accidents and meeting the most obvious regulatory obligations. Yet health challenges have expanded considerably: addictions, chronic fatigue, musculoskeletal disorders (MSDs), sleep disorders, stress-related conditions, sedentary lifestyles… Issues that are less spectacular than a serious accident, but with a major human and economic cost. A modern occupational health policy can no longer be limited to ticking boxes: it must address these dimensions in a global, coordinated way.
Addictions are a first area requiring vigilance. Alcohol, illicit drugs, but also certain medications—and more recently excessive consumption linked to activities such as gambling or certain digital uses—can have a direct impact on safety (driving, operating machinery, working at height, technical interventions) and on work quality. Companies sometimes hesitate to address these topics head-on, for fear of stigmatizing employees or intruding into private life. Yet inaction exposes the organization to major risks. An appropriate policy combines information, prevention, support, and—when safety is directly at stake—strict control of certain situations (alcohol in safety-critical roles, testing in very high-risk sectors, procedures in cases of dangerous behavior).

Fatigue and sleep disorders, often underestimated, form a second critical axis. Shift work, night work, rotating schedules, on-call duty, long commuting times, chronic overload, intrusive digital tools—there is no shortage of factors that disrupt physiological rhythms. The consequences are well known: reduced alertness, errors, irritability, accidents, and longer-term cardiovascular disease. A modern occupational health policy must examine how working hours, on-call arrangements, and daily time spans are organized, as well as connection practices outside working time. When implemented seriously, the right to disconnect becomes a genuine prevention tool.
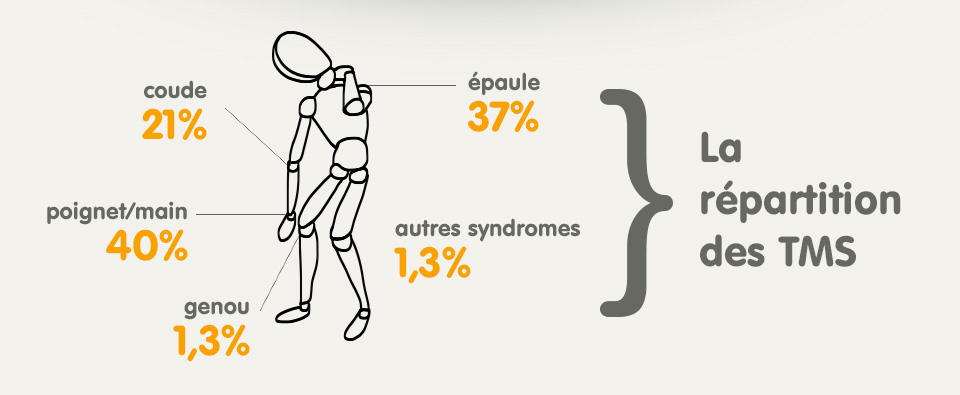
Musculoskeletal disorders, finally, have for years been one of the leading recognized occupational diseases. They are not limited to physically demanding jobs: repetitive gestures, prolonged postures, screen work, and stress also contribute to MSDs in office roles. Effective prevention requires a detailed analysis of workstations, adapted equipment, reflection on work organization (task rotation, breaks), and employee awareness of bodily warning signs. Ergonomics should be seen as a long-term investment, not as optional comfort.
To address these three dimensions—addictions, fatigue, MSDs—in a coherent way, it is helpful to integrate them into a global occupational health policy rather than tackling them through one-off campaigns. Such a policy first requires a clear commitment from leadership, formalized in an accessible, understandable document: What are the company’s values regarding health? How far is it willing to go to protect employees? Which behaviors does it consider unacceptable in terms of endangering oneself or others? When this clarification is clearly stated and assumed, it prevents the ambiguity that fuels tolerance of risky situations.
HR plays a key role in building this policy. HR can connect health issues with working-time management, career paths, workload, and mobility. HR can integrate occupational health criteria into project evaluations, negotiations with employee representatives, and the design of agreements (part-time work, remote work, night work, senior employees). HR is also a major relay for access to support mechanisms: partnerships with addiction-specialist organizations, setting up listening/support hotlines, and employee assistance programs.
Occupational health services—internal or external—remain essential partners, yet they are still too often underused on these topics. Their medical expertise, their understanding of the links between work organization and health conditions, and their perspective on individual cases make them indispensable. A modern health policy seeks to involve them upstream of projects (reorganizations, new schedules, introduction of technologies) rather than downstream, once problems have already emerged. Regular exchanges between HR, managers, health services, and employee representatives help identify weak signals earlier.
Frontline managers are not doctors, but they are often the first to see concrete effects: fatigue, unusual absenteeism, expressed pain, rising tensions. To enable them to act without feeling helpless, they need training in the basics of occupational health: understanding MSD risk factors, knowing how to adjust a workstation, spotting risky behavior, addressing a sensitive topic with an employee, and directing them to the right contacts. Putting managers on the front line without support or training is a common mistake that can backfire on both managers and employees.

Finally, a modern occupational health policy requires accepting that these topics must be discussed without taboo. Addictions, fatigue, and pain are not individual weaknesses that everyone should manage alone. They are human and professional realities present in every environment. By addressing them respectfully, without judgment, and by offering solutions rather than looking for culprits, the company builds a climate of trust. That climate is essential so employees feel able to raise difficulties before they turn into accidents, long-term sick leave, or breakdown situations.



Comments